


Payer mix is a function of the number of patients you have for each payer and how much each payer reimburses at the CPT® code level. The first step to understanding payer mix is to look at your active patient panel size by payer.
Look at both the total number of patients and the total number of visits for the past year, preferably two years. Keep in mind that there may be several plans (products) with different fee schedules under each payer, so do your counts at the plan (product) level.
It’s also essential to compare how much each plan reimburses for your most frequently billed CPT® codes. Knowing what different payers reimburse for the same service (CPT® code) is a critical step to understanding payer mix.
KNOWING – AND MANAGING – YOUR PAYER MIX IS CRITICAL AND HAS A SIGNIFICANT IMPACT ON YOUR BOTTOM LINE
Negotiating better fees is one option for improving your payer mix. Your leverage increases if you have a successful practice. Using the example below, you can give Payer B an option: “Increase our reimbursements, or we will limit our panel size.” If Payer B won’t give an across-the-board increase, ask for greater reimbursement for your most frequently used CPT® codes and/or those where Payer B is below market rate.
Another tactic is to recruit patients who have better-paying insurance, either by targeting zip codes where Payer C patients congregate or employers who offer Payer C to their employees. Asking patients to refer friends and family members remains effective in our social media world.
Here are four examples of a day in which a physician sees 25 established patients in the clinic. The same CPT® code, 99213, is used on all patients. The only difference is the payer mix.
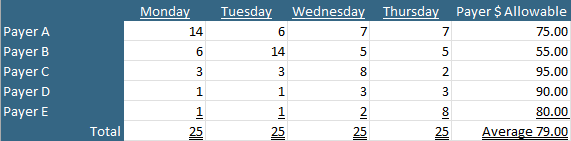
In each example, the same number of patients are seen. The total charges are the same. The same resources are used. The time spent is similar. These four days differ only in payer mix, and consequently so does revenue.
The only difference between Monday and Tuesday is the number of patients seen who have either Payer A or Payer B insurance. The physician has a higher number of patients with Payer A, which pays better than Payer B, on Monday, meaning the physician earns $160 (9.6 percent) more than on Tuesday.
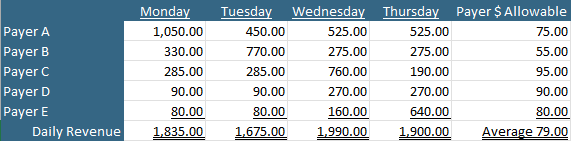
Similarly, Wednesday and Thursday differ only in the number of patients seen who have either Payer C or E. Wednesday includes more patients with the better-paying Payer C and thus produces more revenue $90 (4.7 percent) than Thursday.
Here’s another layer of complexity. Both Wednesday and Thursday generated more revenue than Monday or Tuesday because Payers C and E reimburse better than either Payer A or B.
Let’s look at the impact over the course of a year (254 weekdays).
A physician working 254 Wednesdays will generate $80,010 (18.9 percent) more than a peer working 254 Tuesdays for the same amount of effort. In other words,
CONCLUSION
Payers don’t apportion equal pay for equal work; therefore it is crucial for your practice to understand who pays what (so your contracts can be re-negotiated more effectively). Knowledge is power and planning is essential.
Payer mix matters, a lot.

